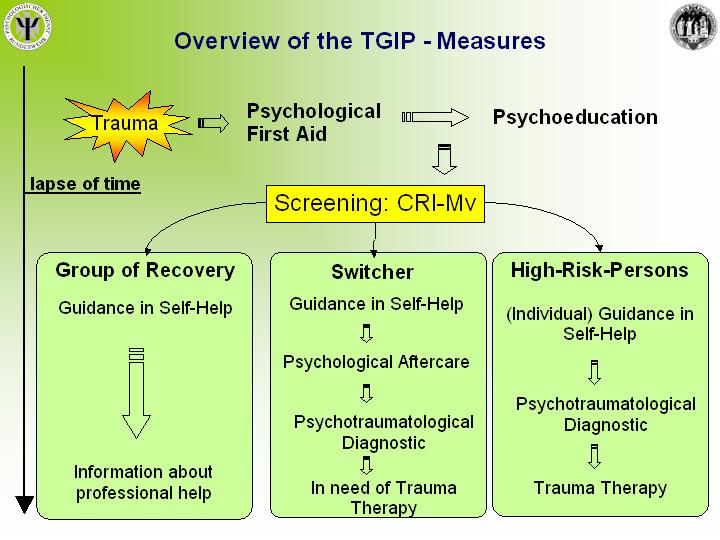
The CRI-Mv Screening forms the basis for the TGIP. According to the risk factors identified persons are assigned to one of three groups:
"Group of Recovery": The persons belonging to the Group of Recovery are likely to cope with the traumatic situation with the use of their given resources and capacities. Their natural healing process is expected to lead to recovery.
"Switchers": The switchers are literally on the verge of chronifying. Whether the traumatic process will lead to recovery or not is significantly influenced by the ammount of additional social and institutional stress imposed on the affected persons during the time following the traumatic situation. Without this additional stress they are likely to come to terms with the traumatic process just as the group of recovery.
"High Risk Group": Persons assigned to the high risk group show a high potential risk of developing a Posttraumatic Stress Disorder or other psychiatric or psychosomatic disorders.
The slide below presents the intervention methods taken for the various groups in accordance with the TGIP. It is taken from the eReader 3.0.
Key Terms:
1. Psychoeducation
An essential step in stabilizing affected persons after a potentially traumatizing situation is giving a Psychoeducation, in which basic knowledge on the traumatic process and the potential effects of traumatic experiences is passed on to the persons affected. This knowledge is intended to support the process of understanding that their reaction is neither insane nor a result of personal failure, but a normal reaction to a crazy situation. Furthermore it has shown to aid the cognitive processing and restructuring of the highly emotional experiences and inexplicable behaviour. It thus counteracts the overwhelming feelings of uncontrollable chaos and enables the persons to distance themselves from those overwhelming feelings.
2. Guidance in self-helping techniques
The affected persons are taught in techniques of calming themselves and taking distance to the traumatic contents which help to control and reduce intrusive traumatic material. These include above all imaginative techniques, exercises of distancing themselves, techniques of relaxation and generally stress reducing behaviour. These measures support the natural healing process and facilitate the step towards the phase of recovery. The main aim of this help is to eventually lead the way to an integration of the traumatic exoperiences into the biographical context and the individual every day life.
3. Psychological Aftercare
Regarding the group of switchers there is a high potential risk that additional stress imposed on the affected person by either their working or social environment or even by their family will cause a PTSD to develop. Owing to the fact that the outcome of the traumatic process is undecided an active form of after care is needed. This could be in the form of a telephone call a few weeks after the screening or a personal meeting with the person. This gives way to an early detection of possibly negative developments and enables the professionals to take the appropriate steps (e.g. trauma therapy) in case needed.
4. Diagnostics
In order to get a more detailled picture of the individual process of dealing with the trauma, the use of diagnostic instruments is indicated. The results also allow a further specification of the treatment needed in each individual case.
Thourough diagnostics should be performed by trained and professional personnel only (i..e. clinical and industrial-organisational psychologists) as extensive knowledge an d experience with Psychotraumatology are imperative (?). Traumadiagnostics include a comprehensive anamnesis as well as a number of traumadiagnostic tests giving an overview over the degree of pretraumatisation and the development of symptoms.